Objective:
Hairy cell leukemia (HCL) is distinct indolent neoplasm of small mature B cells accounting for 2% of the lymphoid leukemias. The classic immunophenotypic profile of HCL includes bright expression of B cell surface antigen and immunoglobulins and lack of both CD5 and CD10. The tumor cells are predominantly present in the spleen, peripheral blood and bone marrow. Aberrant expression of CD5 and lymph node involvement are very rare. A case of CD5(+) HCL with a documentedBRAF V600Emutation has not been previously reported. This case is also unique due to lymph node involvement by HCL. To our knowledge, this is the only case report of a documentedBRAF V600Emutated CD5(+) HCL along with lymph node involvement in the literature.
Method:
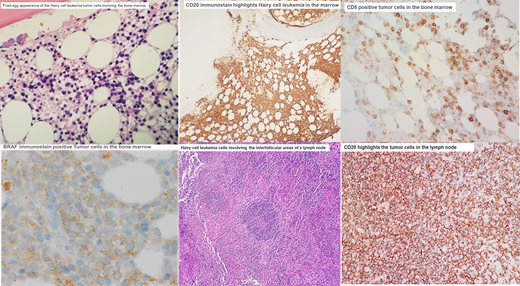
We are presenting a 45 years old man with multiple prior medical conditions including diabetes, COPD and interstitial pneomonitis with new onset of B-symptoms and neutropenia/monocytopenia. Peripheral blood flow cytometry revealed 21% CD5(+) CD10(-) monoclonal B cell population. Further workup revealed the neoplastic cells are positive for CD11c, CD103 and CD25. Bone marrow study revealed an extensive involvement of the marrow.By immunohistochemistry, the cells are also positive for CD5, CD20, BRAF and cyclin D1. Cytogenetic studies show that the cells are negative t(11;14) and molecular studies revealedBRAF V600Emutation. Reexamination of the prior wedge lung resection revealed intrathoracic lymph node involvement.
Results and conclusion:
The most common differential diagnoses of a CD5(+) B cell lymphoma involving the bone marrow is chronic lymphocytic leukemia (CLL) and mantle cell lymphoma. The key into the diagnosis of this case was marked monocytopenia that lead to addition of HCL antibody tubes despite the CD5 positivity and detection of CD25, CD103 and CD11c antigens in the leukemic cells. Bone marrow biopsy show extensive involvement by a CD5(+) cyclin D1(+) B cell lymphoma. The most important differential diagnosis in this case was mantle cell lymphoma. The diagnosis of HCL was confirmed by detection ofBRAF V600Emutation and absence of t (11;14). Retrospective examination of the intrathoracic lymph nodes show one lymph node involvement by hairy cell leukemia cells.
The patient was treated with Vemurafenib and his follow up flow cytometry revealed only 0.60% leukemic involvement. Incorporation of clinical data at the time of flow cytometric examination is essential to aid the hematopathologist in having a broader differential diagnoses and addition of appropriate tests that lead to the more accurate diagnosis and treatment.
No relevant conflicts of interest to declare.